
Let’s Talk Data: Measurement-Based Care at McCallum Place
Since 2013, McCallum Place has collected in-house data to investigate treatment effectiveness, allowing us to better understand eating disorder pathology and improve treatment outcomes. Another name for this process is measurement-based care, which is defined as using client data collected throughout treatment to inform clinical care. While data collection results help determine our specific program effectiveness, McCallum Place data has also helped inform national eating disorder specific grants, programs, and clinics. We are honored to play a role in developing literature and research that fosters new programing, laws, and clinical approaches.
So what does measurement-based care look like at McCallum Place? It is our standard practice to administer behavioral assessments to our patients throughout their treatment stays. Assessment is provided to new patients within one week of their admission date, every 30 days throughout their treatment stay, and before discharge. We also follow up with patients after discharge through online surveys which are emailed at: 1 month, 3, 6, 12, 18, and 24. At McCallum place we utilize the following measures:
- Eating Disorder Examination Questionnaire (EDE-Q; Fairburn & Beglin, 1994),
- Eating Pathology Symptoms Inventory (EPSI; Forbush, Wildes, Pollack, Dunbar, Patterson, et al., 2015),
- Clinical Impairment Assessment (CIA; Bohn & Fairburn, 2008),
- Penn State Worry Questionnaire (PSWQ-10; Yao, Sripada, Klumpp, Abelson, Muzik, Zhao, et al., 2016),
- Inventory of Depression and Anxiety Symptoms (IDAS; Watson, Simms, Kotov, & Chmielewski, 2007),
- Obsessive Compulsive Inventory-Revised (OCI-R; Foa, Huppert, Leiberg, Hajcak, Langner, et al., 2002), and
- Compulsive Exercise Test (CET; Taranis, Touyz, & Meyer, 2011)
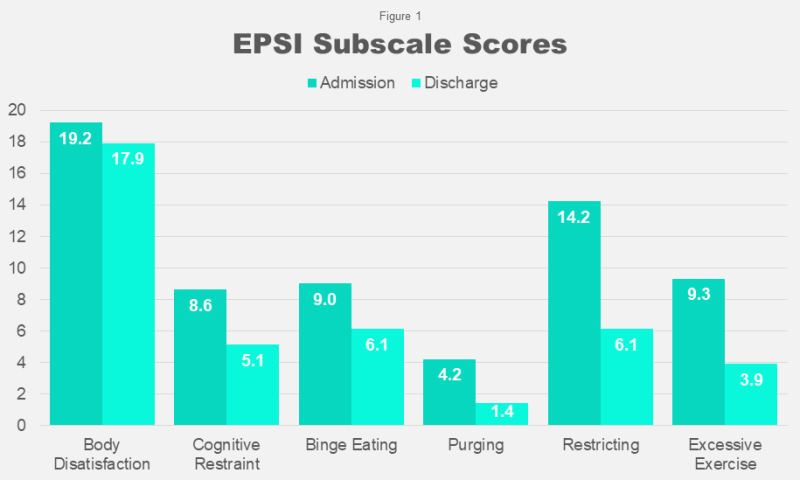
We use this data, collected in surveys, in a few different ways. Primarily all the data gets pooled to generate average scores. Then, we evaluate score changes throughout treatment stays and post-discharge. In other words, we examine the average scores of each survey at admission compared to discharge, compared to after discharge. This helps us observe how effective treatment is overall. For instance, in Figures 1-3 you can see how the average scores change for our 2013 to 2019 patients from admission to discharge. Figure 1 demonstrates the changes in eating disorder symptoms measured by the Eating Pathology Symptoms Inventory, and Figure 2 demonstrates the changes in depression and anxiety symptoms measured by the Inventory of Depression and Anxiety Symptoms—all score changes from admission to discharge were statistically significant beyond p<.001.
What does that mean, you ask? Well, statistical significance is how we quantify if a data result happened by chance. If a result is statistically significant that means it is very unlikely that you found that result due to chance. “Beyond p<.001” refers to the p-value, which is the numerical cutoff that tells us if a data finding is statistically significant. A p-value of .05 or less (p<.05) means the result is statistically significant, and p-value greater than .05 (p>.05) means the result is not statistically significant.
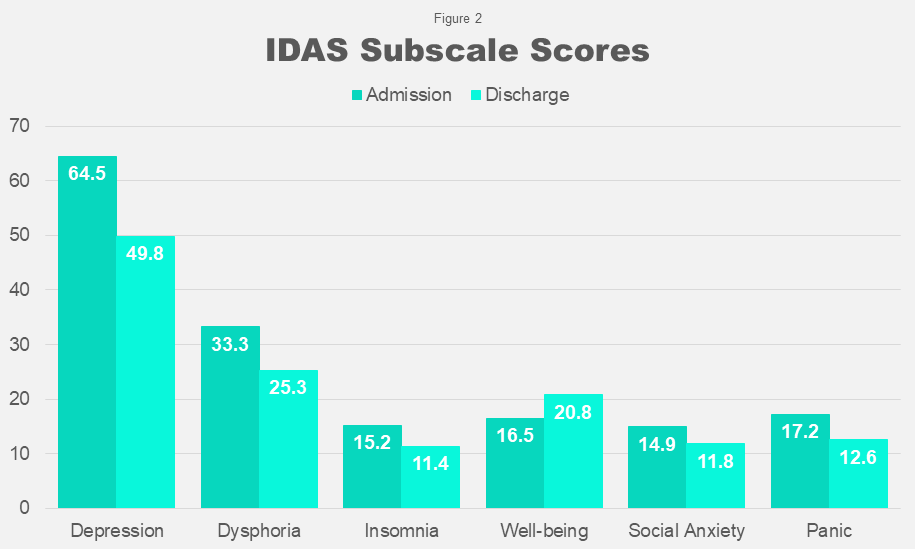
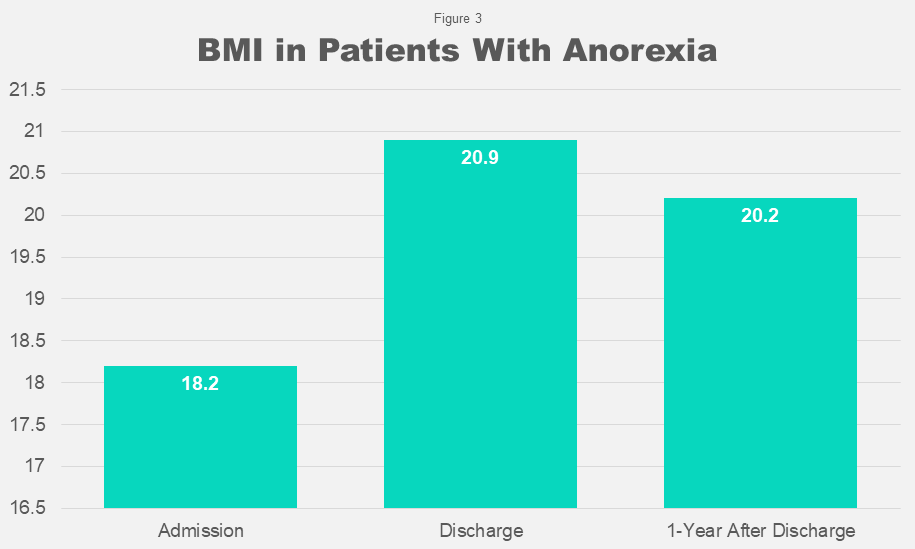
Figure 3 shows the change in average BMI in our admitted patients with Anorexia from admission to discharge, which was statistically significant beyond p<.001. Figure 3 also shows the average BMI of those same patients 1-year after discharge, with no statistically significant (p>.05) change in BMI. This demonstrates that our patients with Anorexia, on average, are maintaining a restored BMI after leaving our care.
Individual patient survey scores can also be used in treatment planning by patients’ treatment providers. Therapists, dietitians, and psychiatrists use their patients’ survey scores to identify areas of focus for treatment—which help us create goals and identify progress during patients’ treatment stays.
An additional and invaluable way data, collected in surveys, gets utilized is through sharing reports with our staff. When survey data is transformed into treatment outcome reports, we share those outcomes with our employees. Every single staff member at McCallum Place plays a vital role in providing treatment to our patients, and our outcomes are a tangible demonstration of the real-life change they facilitate in their day-to-day work.
As a treatment facility with robust data collection, we are frequently asked about our recovery rates. We understand that choosing intensive treatment is an overwhelmingly difficult decision, and having confidence in the effectiveness of that potential treatment is priceless. We would also be remiss to say that while measurement-based care is incredibly important, survey scores do not provide a complete picture of a person. People are not their symptoms or a number. Conversely, data does not predict an absolute outcome. In fact, outcomes are not often measured in the same ways across eating disorder treatment or research. This is why we do not claim that our treatment has a percent of recovered or unrecovered patients. Instead we report our outcomes as they are, statistically significant (or not) improvements over the course of treatment and beyond. We are extremely grateful that our data, when examined from 2013 to present as a whole, does indeed demonstrate statistically significant improvements across each symptom domain we measure here at McCallum Place, and we are always more than happy to share as much about those findings with anyone who asks. If you have any questions about the research we conduct at McCallum Place, the data shared in this blog, or anything else, please feel free to reach out!




