In Vermont, Where Almost Everyone Has Insurance, Many Can’t Find or Afford Care

RICHMOND, Vt. — On a warm autumn morning, Roger Brown walked through a grove of towering trees whose sap fuels his maple syrup business. He was checking for damage after recent flooding. But these days, his workers’ health worries him more than his trees’.
The cost of Slopeside Syrup’s employee health insurance premiums spiked 24% this year. Next year it will rise 14%.
The jumps mean less money to pay workers, and expensive insurance coverage that doesn’t ensure employees can get care, Brown said. “Vermont is seen as the most progressive state, so how is health care here so screwed up?”
Vermont consistently ranks among the healthiest states, and its unemployment and uninsured rates are among the lowest. Yet Vermonters pay the highest prices nationwide for individual health coverage, and state reports show its providers and insurers are in financial trouble. Nine of the state’s 14 hospitals are losing money, and the state’s largest insurer is struggling to remain solvent. Long waits for care have become increasingly common, according to state reports and interviews with residents and industry officials.
Rising health costs are a problem across the country, but Vermont’s situation surprises health experts because virtually all its residents have insurance and the state regulates care and coverage prices.
For more than 15 years, federal and state policymakers have focused on increasing the number of people insured, which they expected would shore up hospital finances and make care more available and affordable.
“Vermont’s struggles are a wake-up call that insurance is only one piece of the puzzle to ensuring access to care,” said Keith Mueller, a rural health expert at the University of Iowa.
Regulators and consultants say the state’s small, aging population of about 650,000 makes spreading insurance risk difficult. That demographic challenge is compounded by geography, as many Vermonters live in rural areas, where it’s difficult to attract more health workers to address shortages.
At least part of the cost spike can be attributed to patients crossing state lines for quicker care in New York and Massachusetts. Those visits can be more expensive for both insurers and patients because of long ambulance rides and charges from out-of-network providers.
Patients who stay, like Lynne Drevik, face long waits. Drevik said her doctor told her in April that she needed knee replacement surgeries — but the earliest appointment would be in January for one knee and the following April for the other.
Drevik, 59, said it hurts to climb the stairs in the 19th-century farmhouse in Montgomery Center she and her husband operate as an inn and a spa. “My life is on hold here, and it’s hard to make any plans,” she said. “It’s terrible.”
Health experts say some of the state’s health system troubles are self-inflicted.
Unlike most states, Vermont regulates hospital and insurance prices through an independent agency, the Green Mountain Care Board. Until recently, the board typically approved whatever price changes companies wanted, said Julie Wasserman, a health consultant in Vermont.
The board allowed one health system — the University of Vermont Health Network — to control about two-thirds of the state’s hospital market and allowed its main facility, the University of Vermont Medical Center in Burlington, to raise its prices until it ranked among the nation’s most expensive, she said, citing data the board presented in September.
Hospital officials contend their prices are no higher than industry averages.
But for 2025, the board required the University of Vermont Medical Center to cut the prices it bills private insurers by 1%.
The nonprofit system says it is navigating its own challenges. Top officials say a severe lack of housing makes it hard to recruit workers, while too few mental health providers, nursing homes, and long-term care services often create delays in discharging patients, adding to costs.
Two-thirds of the system’s patients are covered by Medicare or Medicaid, said CEO Sunny Eappen. Both government programs pay providers lower rates than private insurance, which Eappen said makes it difficult to afford rising prices for drugs, medical devices, and labor.
Officials at the University of Vermont Medical Center point to several ways they are trying to adapt. They cited, for example, $9 million the hospital system has contributed to the construction of two large apartment buildings to house new workers, at a subsidized price for lower-income employees.

The hospital also has worked with community partners to open a mental health urgent care center, providing an alternative to the emergency room.
In the ER, curtains separate areas in the hallway where patients can lie on beds or gurneys for hours waiting for a room. The hospital also uses what was a storage closet as an overflow room to provide care.
“It’s good to get patients into a hallway, as it’s better than a chair,” said Mariah McNamara, an ER doctor and associate chief medical officer with the hospital.

For the about 250 days a year when the hospital is full, doctors face pressure to discharge patients without the ideal home or community care setup, she said. “We have to go in the direction of letting you go home without patient services and giving that a try, because otherwise the hospital is going to be full of people, and that includes people that don’t need to be here,” McNamara said.
Searching for solutions, the Green Mountain Care Board hired a consultant who recommended a number of changes, including converting four rural hospitals into outpatient facilities, in a worst-case scenario, and consolidating specialty services at several others.
The consultant, Bruce Hamory, said in a call with reporters that his report provides a road map for Vermont, where “the health care system is no match for demographic, workforce, and housing challenges.”
But he cautioned that any fix would require sacrifice from everyone, including patients, employers, and health providers. “There is no simple single policy solution,” he said.
One place Hamory recommended converting to an outpatient center only was North Country Hospital in Newport, a village in Vermont’s least populated region, known as the Northeast Kingdom.


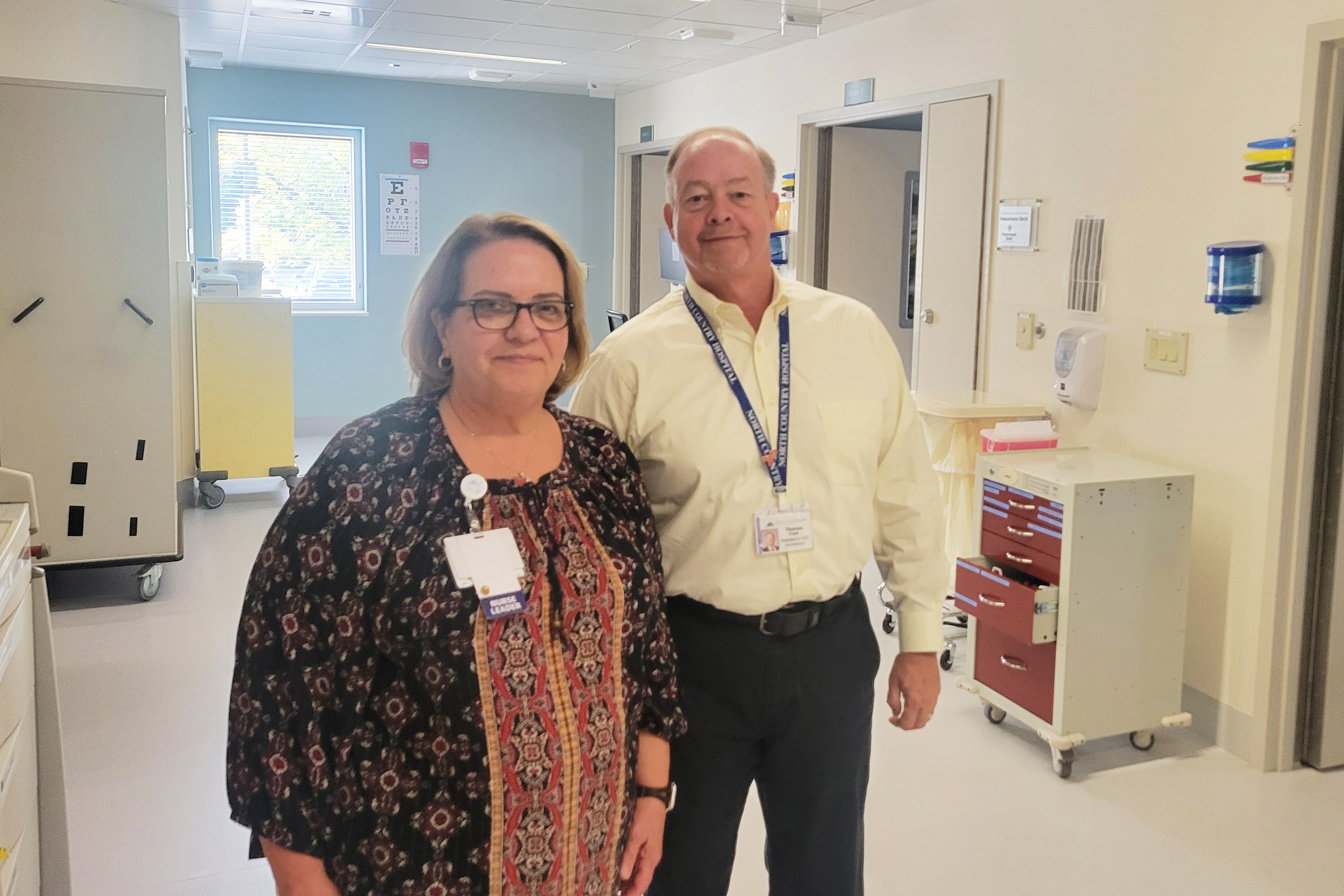
The 25-bed hospital has lost money for years, partly because of an electronic health record system that has made it difficult to bill patients. But the hospital also has struggled to attract providers and make enough money to pay them.
Officials said they would fight any plans to close the hospital, which recently dropped several specialty services, including pulmonology, neurology, urology, and orthopedics. It doesn’t have the cash to upgrade patient rooms to include bathroom doors wide enough for wheelchairs.
On a recent morning, CEO Tom Frank walked the halls of his hospital. The facility was quiet, with just 14 admitted patients and only a couple of people in the ER. “This place used to be bustling,” he said of the former pulmonology clinic.
Frank said the hospital breaks even treating Medicare patients, loses money treating Medicaid patients, and makes money from a dwindling number of privately insured patients.
The state’s strict regulations have earned it an antihousing, antibusiness reputation, he said. “The cost of health care is a symptom of a larger problem.”
About 30 miles south of Newport, Andy Kehler often worries about the cost of providing health insurance to the 85 workers at Jasper Hill Farm, the cheesemaking business he co-owns.
“It’s an issue every year for us, and it looks like there is no end in sight,” he said.

Jasper Hill pays half the cost of its workers’ health insurance premiums because that’s all it can afford, Kehler said. Employees pay $1,700 a month for a family, with a $5,000 deductible.
“The coverage we provide is inadequate for what you pay,” he said.